Glaucoma is a group of eye conditions that damage the optic nerve, which carries visual information from the eye to the brain. The most common form, primary open-angle glaucoma, usually develops slowly and may cause no obvious symptoms in its early stages. Raised pressure inside the eye is an important risk factor, but glaucoma can also occur when pressure readings are within a typical range, and high pressure does not always mean that glaucoma is present.
Because symptoms and a single pressure measurement cannot confirm or exclude glaucoma, detection relies on a comprehensive eye examination and a combination of tests.
Go to the nearest emergency department or call triple zero (000) if an eye quickly becomes severely painful and red and vision becomes blurred or surrounded by halos, particularly if headache, nausea or vomiting is also present.
These symptoms may indicate acute angle-closure glaucoma. Do not wait for a routine eye appointment.
What is glaucoma?
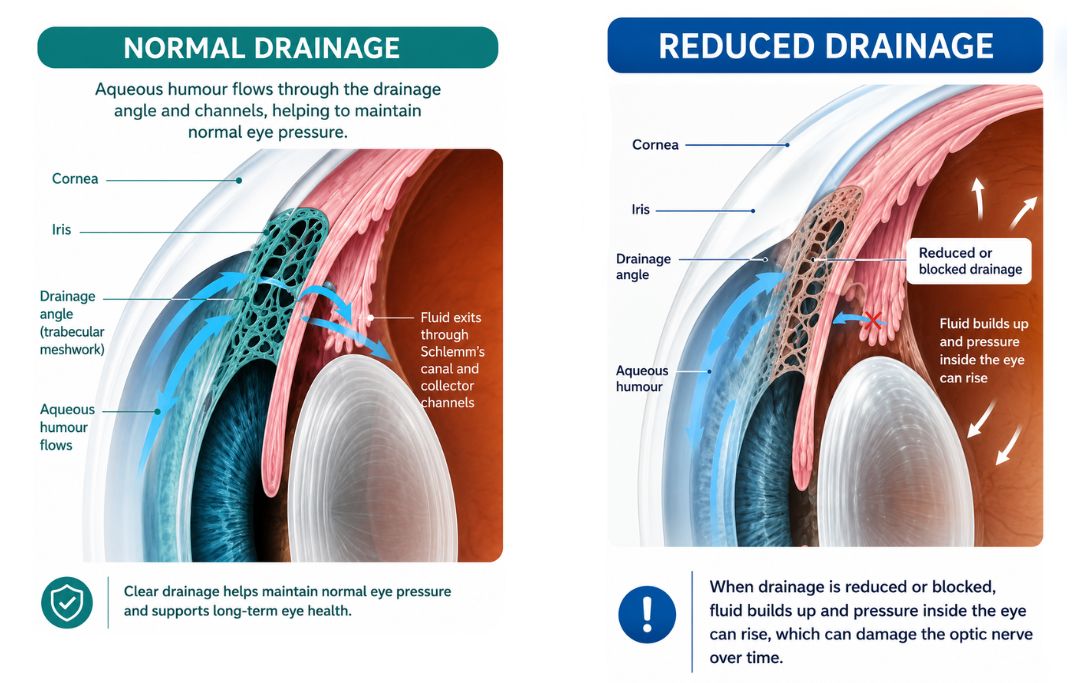
The front of the eye contains a clear fluid called aqueous humour. This fluid is continually produced and normally drains through channels near the front of the eye. If drainage is reduced, pressure inside the eye may rise. Pressure that is too high for a person’s optic nerve can contribute to damage, although eye pressure is only one part of the condition.
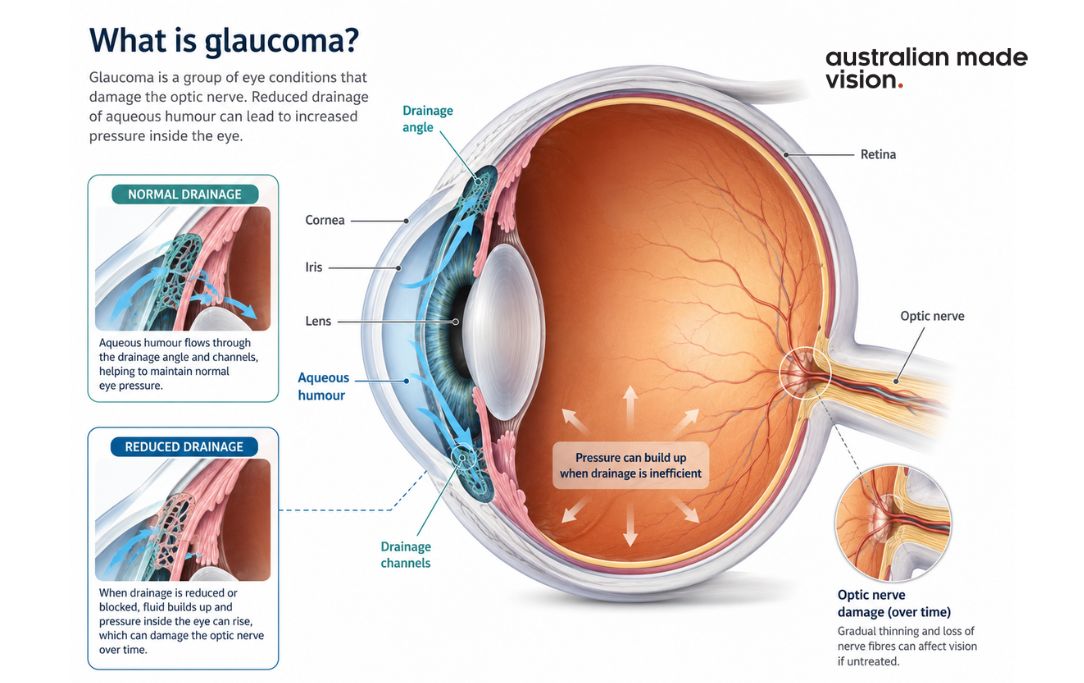
Glaucoma damages the optic nerve over time. The changes may affect peripheral, or side, vision first. Without treatment, the damaged area of vision can expand. Vision already lost because of glaucoma generally cannot be restored, so the aim of assessment and treatment is to identify the condition and limit further damage.
Primary open-angle glaucoma
Primary open-angle glaucoma is the most common form in Australia. The eye’s drainage angle remains open, but fluid does not drain efficiently enough to maintain a pressure that is safe for the optic nerve. The condition usually progresses gradually, which is why many people do not notice a change during the early stages.
Acute angle-closure glaucoma
Angle-closure glaucoma occurs when the eye’s drainage pathways become narrowed or blocked. In an acute attack, eye pressure can rise quickly. Symptoms may include severe eye pain, redness, blurred vision, halos around lights, headache, nausea or vomiting. Acute angle-closure glaucoma requires immediate medical assessment.
Other types of glaucoma
Secondary glaucoma can develop because of another eye condition, an eye injury, previous eye surgery or certain medicines. Less common developmental forms can occur in babies or children. The tests and treatment pathway depend on the type of glaucoma and the individual examination findings.
Is Your Eye
Health on Track?
Complete our free 18-point checklist to check your eye health, spot any gaps, and take charge of your vision.
Start Free Checklist Test →What are the symptoms of glaucoma?
Primary open-angle glaucoma may not cause noticeable symptoms at first. Small areas of peripheral vision can be affected without the person being aware of the change. As damage progresses, the field of vision may become more restricted.
Chronic angle-closure glaucoma may also produce few symptoms, although some people notice intermittent blurred vision or halos around lights. These symptoms can have several possible causes, so an eye examination is needed rather than assuming glaucoma is responsible.
A sudden painful red eye with blurred vision or halos, especially when accompanied by headache, nausea, or vomiting, is different. These symptoms may indicate acute angle-closure glaucoma and need emergency assessment.
Glaucoma is only one possible cause, and professional assessment is needed to identify what may be contributing to the change.
Who is at higher risk of glaucoma?
Anyone can develop glaucoma, but some factors are associated with a higher risk. Having one or more risk factors does not mean that glaucoma is certain, and having no known risk factors does not rule it out.
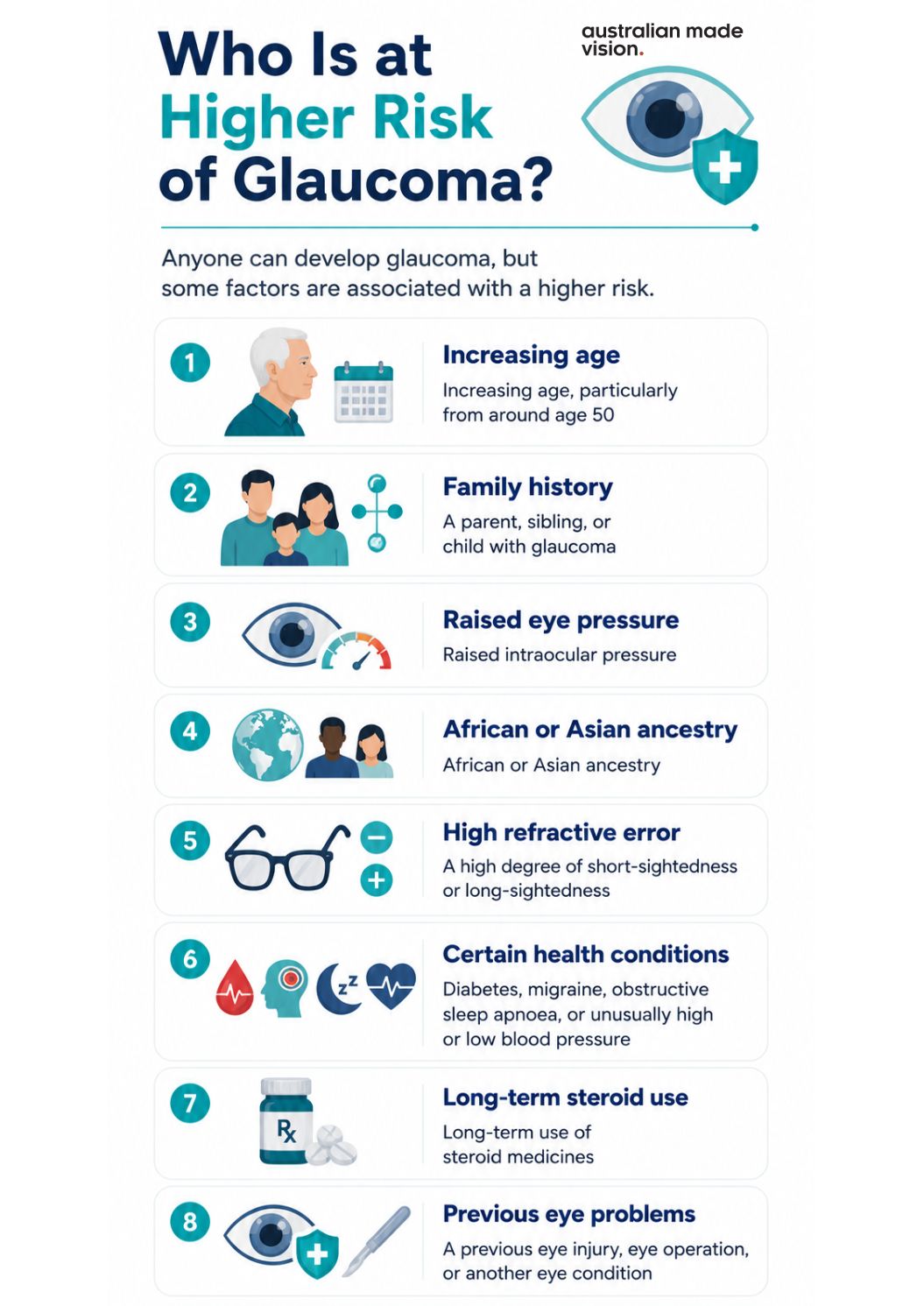
- increasing age, particularly from the age of 50
- a parent, sibling or child with glaucoma
- raised intraocular pressure
- African or Asian ancestry
- a high degree of short-sightedness or long-sightedness
- diabetes, migraine, obstructive sleep apnoea or a history of unusually high or low blood pressure
- long-term use of steroid medicines
- a previous eye injury, eye operation or another eye condition
Family history is particularly useful information to share with an optometrist or ophthalmologist. If a close relative has glaucoma, ask an eye-care professional when comprehensive examinations should begin and how often they are appropriate for your circumstances.
Find Eye Care That Suits Your Needs
Search for an independent optometrist near you and find a local practice that suits your specific eye care needs.
Find an OptometristHow is glaucoma detected?
Glaucoma cannot be confirmed through symptoms alone. It is also not diagnosed from one eye-pressure reading. An optometrist or ophthalmologist may combine several findings to assess the optic nerve, the eye’s drainage system and the person’s field of vision.
Health and family history: The practitioner may ask about glaucoma in close relatives, previous eye injuries or operations, medical conditions, and medicines, including steroid use.
Eye-pressure measurement: Tonometry measures intraocular pressure. A high result can increase concern, but the reading must be considered with the rest of the examination.
Optic nerve examination: The optic nerve is checked for changes that may be associated with glaucoma. Pupil-dilating drops may be used when a wider view of the back of the eye is needed.
Drainage-angle assessment: Gonioscopy allows the practitioner to examine whether the drainage angle is open, narrow or closed. This can help distinguish between different forms of glaucoma.
Visual-field testing: Perimetry checks central and peripheral vision one eye at a time. The results can help identify patterns of vision loss and can be compared with later tests.
Optical coherence tomography: OCT imaging can measure the retinal nerve fibre layers around the optic nerve. It may help document structure and monitor change when the equipment is available and the test is clinically appropriate.
Corneal-thickness measurement: Pachymetry measures the thickness of the cornea. Corneal thickness can affect how an eye-pressure result is interpreted.
The practitioner may need to compare results over time, particularly when the changes are subtle or the person is considered a glaucoma suspect. The tests offered, their availability and any additional fees vary between practices.
What happens if glaucoma is suspected?
An optometrist may identify an unusual optic nerve appearance, raised eye pressure, a visual-field change, or another finding that requires further investigation. Depending on the results, the optometrist may recommend referral to an ophthalmologist for diagnosis, treatment decisions or specialist monitoring.
A person may be described as a glaucoma suspect when some findings raise concern but the diagnosis is not yet clear. This does not necessarily mean that glaucoma is present. Repeated eye-pressure measurements, optic nerve images, OCT scans, or visual-field tests may be used to look for change over time.
Follow-up timing is individual. It depends on the examination findings, the person’s risk factors and the plan recommended by the treating optometrist or ophthalmologist. People already asked to attend monitoring appointments should not wait for symptoms before returning, because open-angle glaucoma can progress without a noticeable change in everyday vision.
Is Your Eye
Health on Track?
Complete our free 18-point checklist to check your eye health, spot any gaps, and take charge of your vision.
Start Free Checklist Test →How is glaucoma treated and managed?
Glaucoma treatment is intended to lower eye pressure and reduce the risk of further optic nerve damage. It cannot restore vision already lost to glaucoma. The appropriate option depends on the type and severity of glaucoma, the person’s health and how the eye responds to treatment.
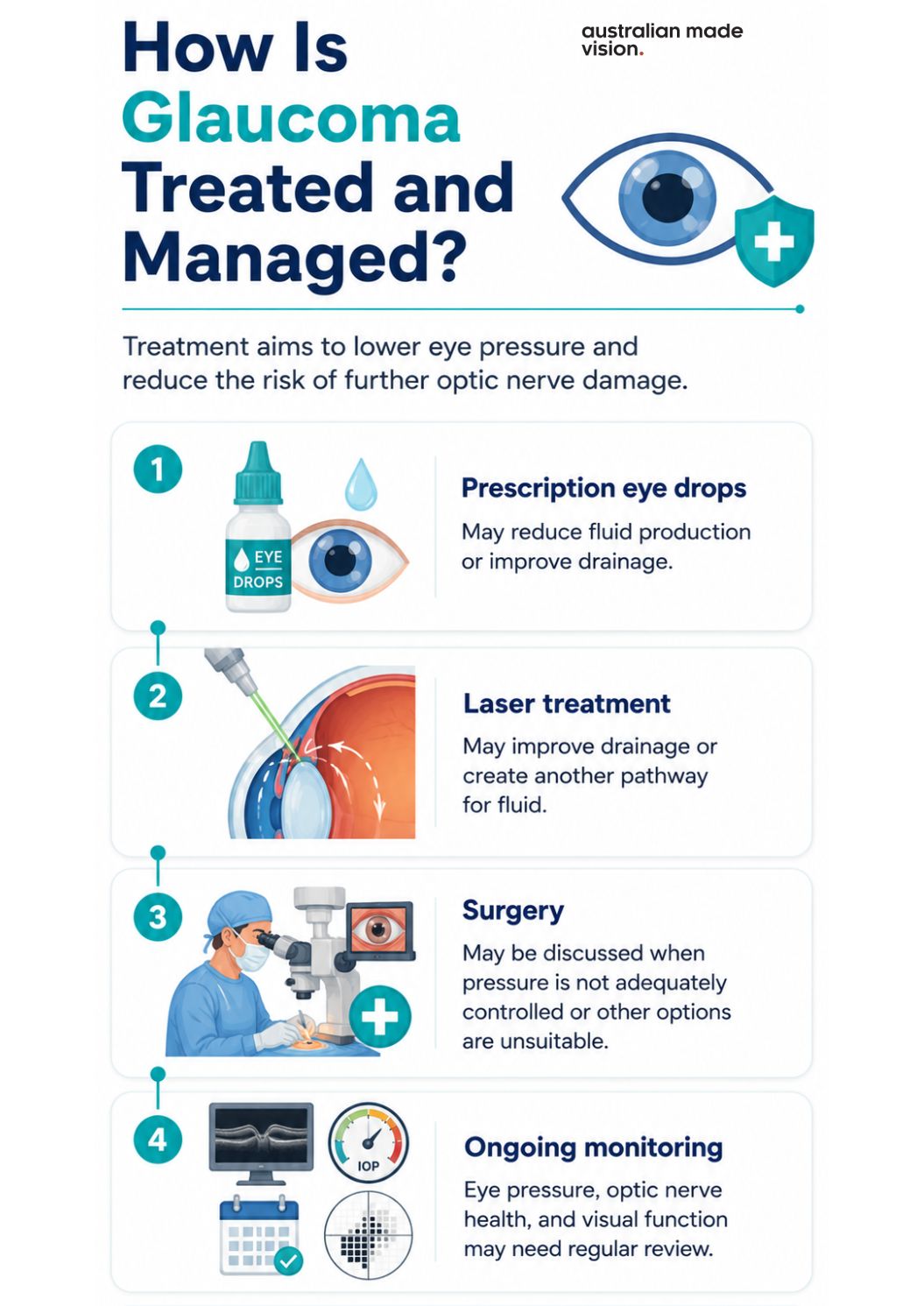
Prescription eye drops: Eye drops are commonly used to reduce the amount of fluid produced in the eye or improve its drainage. They should be used exactly as prescribed. Questions about side effects, technique, or missed doses should be discussed with the prescribing clinician or pharmacist.
Laser treatment: Different laser procedures may be used for open-angle or angle-closure glaucoma. The purpose may be to improve drainage or create another pathway for fluid, depending on the type of glaucoma.
Surgery: An ophthalmologist may discuss surgery when pressure is not adequately controlled, when other options are unsuitable or when the clinical situation requires it. Several surgical approaches are available, including less invasive, and conventional procedures.
Ongoing monitoring: Treatment is not a substitute for follow-up. Eye pressure, the optic nerve, and visual function may need to be reviewed so the treating team can assess whether the condition is stable or changing.
Do not stop or change prescribed glaucoma treatment without speaking with the clinician responsible for your care. Treatment plans vary, and advice that is appropriate for one person may not be suitable for another.
Questions to ask before a glaucoma assessment
Services and equipment vary between practices. These questions can help you understand what an appointment may involve and whether further referral could be needed:
- Does this practice provide a comprehensive glaucoma assessment, and which tests may be needed?
- Are optic nerve imaging and visual-field tests available, and can additional fees apply?
- How will my results be recorded and compared with future examinations?
- When would referral to an ophthalmologist be recommended?
- Based on my age, family history, and other risk factors, when should I be reviewed?
- If glaucoma is confirmed, which clinician will manage treatment and ongoing monitoring?
When should you arrange eye care?
Routine eye care: If you have a family history of glaucoma, have been told that your eye pressure is high or have another recognised risk factor, discuss an appropriate examination schedule with an optometrist or ophthalmologist. The timing should reflect your individual risk and previous findings.
Prompt assessment: Arrange an eye examination for persistent or unexplained changes in vision. Blurred vision, halos or reduced side vision can have several causes and should not be self-diagnosed.
Emergency care: Go to the nearest emergency department or call triple zero (000) if an eye quickly becomes severely painful and red and vision becomes blurred or surrounded by halos, particularly if headache, nausea or vomiting is also present.
Finding an optometry practice for routine glaucoma checks
Glaucoma can be difficult to notice without an eye examination. If you have a family history, another recognised risk factor or a recommended review that is due, contact an individual optometry practice and ask which glaucoma-related assessments are available. Services, equipment and fees vary, so confirm the details directly with the practice.
Use the Australian Made Vision directory to find an independent optometrist. Confirm directly with the individual practice which glaucoma-related services, tests and fees apply.
Australian Made Vision provides general eye-health information and a directory of participating independent practices. It does not provide examinations, diagnoses or treatment. Emergency symptoms require emergency care rather than a directory search.
Find Eye Care That Suits Your Needs
Search for an independent optometrist near you and find a local practice that suits your specific eye care needs.
Find an OptometristGlaucoma FAQs
What are the first signs of glaucoma?
The most common form of glaucoma often has no obvious early signs. Peripheral vision may be affected gradually, and the change can be difficult to notice. Acute angle-closure glaucoma is different and may cause sudden severe eye pain, redness, blurred vision, halos, headache, nausea or vomiting.
Can an optometrist detect glaucoma?
An optometrist can assess for signs and risk factors using a combination of tests, such as eye-pressure measurement, optic nerve examination and visual-field testing. Referral to an ophthalmologist may be recommended when glaucoma is suspected or when specialist diagnosis and treatment are needed.
Does normal eye pressure rule out glaucoma?
No. Some people develop glaucoma even when their pressure readings are within a typical range. Eye pressure is one part of the assessment and must be considered with the appearance of the optic nerve, visual-field results and other findings.
Is glaucoma hereditary?
Glaucoma can run in families. A close relative with glaucoma is a recognised risk factor, so it is worth telling your optometrist or ophthalmologist about your family history and asking when you should be examined.
Can glaucoma be cured or reversed?
There is no cure that restores optic nerve damage or vision already lost to glaucoma. Treatment can lower eye pressure and may slow or prevent further damage. Ongoing monitoring remains important even when the condition appears stable.
What symptoms of acute angle-closure glaucoma require emergency care?
Sudden severe eye pain, a red eye, blurred vision or halos around lights, especially with headache, nausea or vomiting, require immediate assessment. Go to the nearest emergency department or call triple zero (000).
Australian Made Vision is an independent directory that helps patients find optometrists across Australia who may offer Australian-made spectacle lenses. We do not provide clinical services and recommend contacting practices directly to confirm the products and services they offer.
