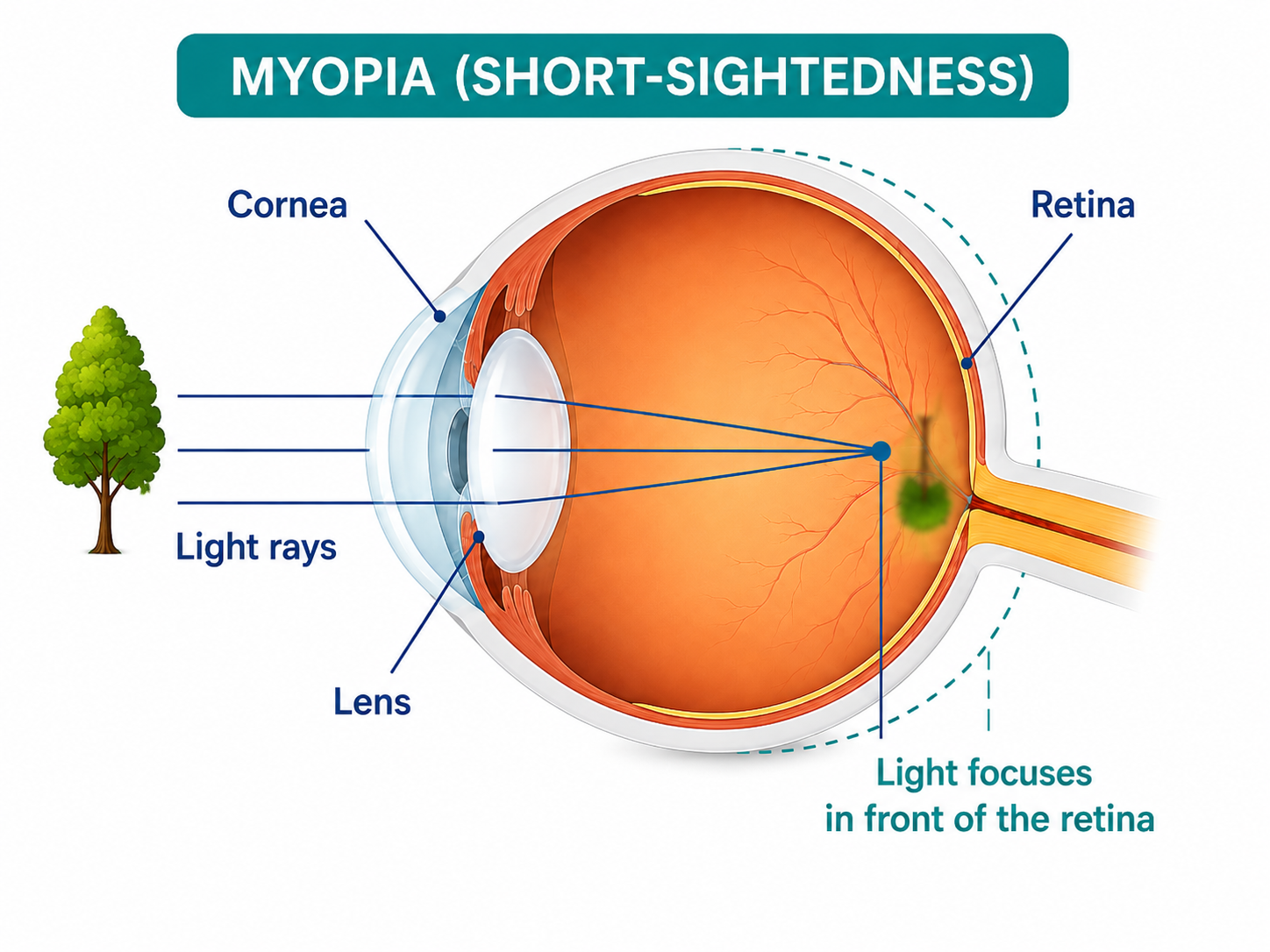
Short-sightedness, also called myopia, is a common refractive error that makes distant objects appear blurred while closer objects may remain clear.
It happens when light entering the eye focuses in front of the retina instead of directly on it. An eye test is needed to confirm whether distance blur is caused by myopia or another eye or health concern.
Prescription glasses or contact lenses can correct blurred vision. For children whose myopia is progressing, an optometrist may also discuss options intended to slow further progression.
These options do not reverse myopia. The most appropriate approach depends on the child, their eyes, their daily routine and the findings from a professional assessment.
Myopia usually causes gradual distance blur.
Go to an emergency department immediately or call triple zero (000) if you experience:
- Sudden vision loss
- new flashes of light
- a sudden increase or change in floaters
- distorted vision
- a shadow or dark curtain across your vision
These symptoms can be associated with retinal detachment and require urgent assessment.
Myopia at a glance
| Question | General answer |
|---|---|
| What does myopia affect? | Mainly distance vision. Road signs, classroom boards and television captions may appear blurred. |
| When does it usually begin? | It often begins in childhood, but it can also develop or continue changing during early adulthood. |
| How is it confirmed? | An optometrist or ophthalmologist assesses vision, refraction and eye health. |
| Can it be corrected? | Yes. Glasses and contact lenses can help focus light correctly on the retina. |
| Can progression be slowed? | Some evidence-based optical and prescription options may slow progression in children. Professional assessment and monitoring are required. |
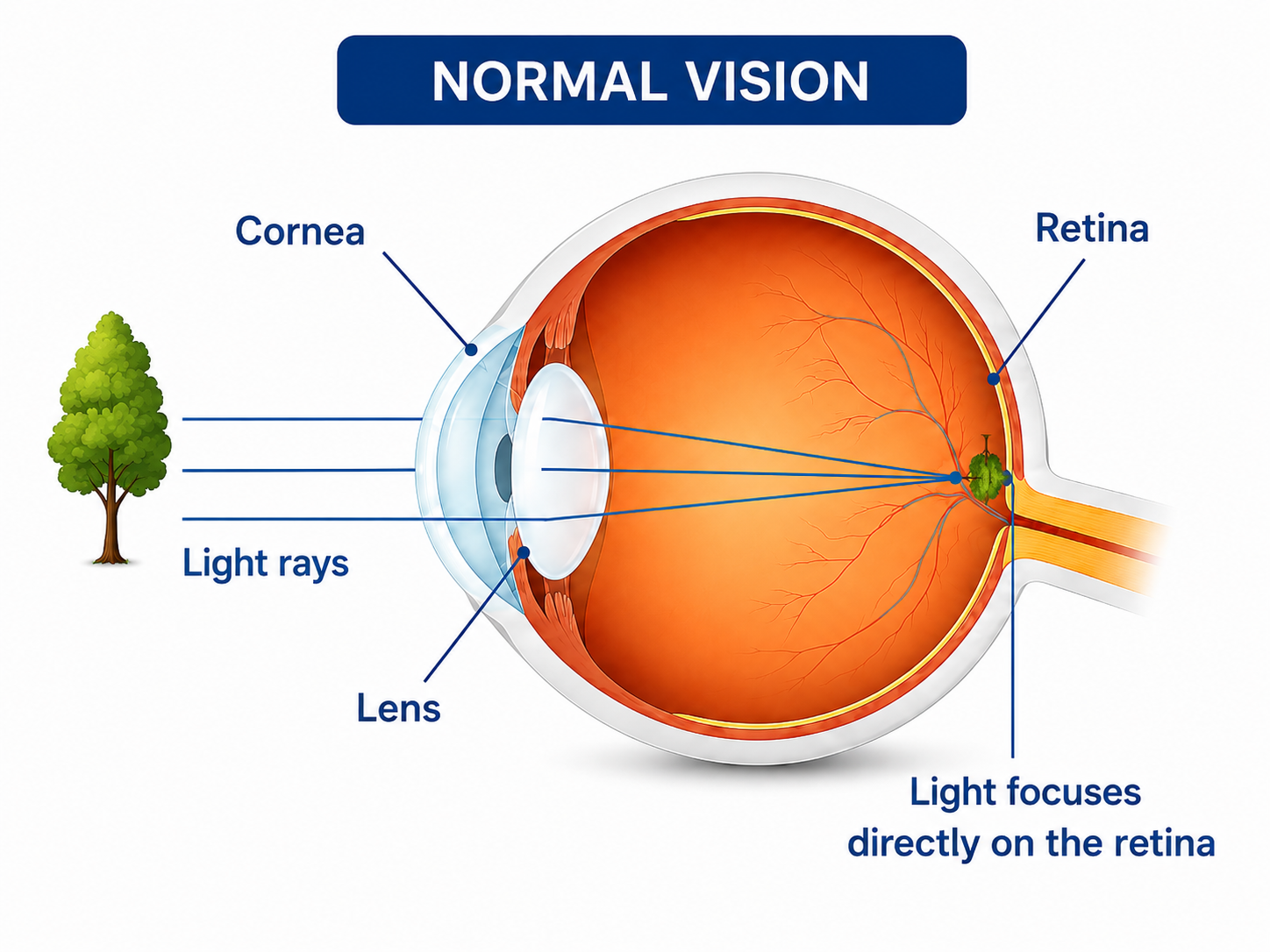
What is myopia?
The cornea and the natural lens at the front of the eye bend incoming light so it can form a clear image on the retina at the back of the eye.
In a myopic eye, the eye may be longer than usual from front to back, or the cornea may have a different curve. Light from distant objects then comes to a focus before it reaches the retina, causing the image to appear blurred.
Myopia is measured in dioptres and is written with a minus sign on an optical prescription. A stronger minus number generally means more correction is needed for clear distance vision.
The prescription shows the focusing correction required. It does not, by itself, provide a complete assessment of the health of the eye.
Myopia often starts during the school years and may change as a child grows. It can also begin later or continue progressing into early adulthood. The timing and rate of progression vary between people.
A new or changing prescription should therefore be professionally assessed rather than assumed to be part of normal growth.
Is Your Eye
Health on Track?
Complete our free 18-point checklist to check your eye health, spot any gaps, and take charge of your vision.
Start Free Checklist Test →Common signs of short-sightedness
The main feature of myopia is blurred distance vision. Other signs may depend on the person’s age, daily activities and prescription.
Signs can include:
- squinting to see road signs, television captions, faces or presentation screens
- difficulty seeing a classroom board or copying information from a distance
- sitting close to the television
- moving closer to distant objects to see more detail
- difficulty recognising people or objects until they are nearby
- difficulty driving when distant detail or low-light vision is unclear
- headaches or tired eyes in some people
Headaches and eye fatigue can have many causes and do not automatically mean someone has myopia.
Children may not realise that their distance vision is different from other people’s. A parent, carer or teacher may instead notice that a child is squinting, moving closer to the board or avoiding activities that rely on clear distance vision.
These signs do not confirm myopia, but they are a reason to arrange an eye test.
What causes myopia?
Myopia is a complex condition influenced by the way the eye grows and by a combination of genetic and environmental factors.
It is not usually possible to identify one single cause for an individual person.
Factors associated with the development or progression of myopia include:
- a family history of myopia
- myopia beginning at a younger age
- less time spent outdoors during childhood
- long periods of close work, including reading, studying and using handheld devices
- individual eye-growth and genetic factors
Screen use should not be described as the only cause of myopia.
Digital devices are one form of close work, and screen-heavy routines may also reduce the time a child spends outdoors. The broader pattern of near work, breaks, outdoor activity, family history and eye growth should be considered.
How is myopia assessed during an eye test?
An optometrist or ophthalmologist can assess myopia as part of an eye examination.
The tests used may vary depending on the person’s age, symptoms, health history and reason for attending.
An assessment may include:
- questions about when the blurred vision started
- discussion of whether the vision is changing
- questions about how the blur affects school, work, driving, or other activities
- distance and near vision testing
- refraction to measure the lens power needed for clear vision
- assessment of eye coordination and focusing
- examination of the health of the front and back of the eyes
- discussion of family history and previous prescription changes
For children who may be at risk of progression, the optometrist may also use cycloplegic refraction or ocular biometry where these tests are clinically appropriate and available.
Measuring the prescription shows how much optical correction is needed. When a child is receiving active myopia management, an optometrist may also monitor changes in the refractive error and, where available, the length of the eye.
The method and timing of follow-up appointments should be selected for the individual child and the management option being used.
You can also read the AMV guide to what to expect during an eye check.
How is myopia corrected?
Myopia correction helps bring light into focus on the retina so distance vision appears clearer.
Correcting the blur does not necessarily change how the eye grows or remove the need to monitor eye health.
Glasses
Prescription spectacle lenses are a common, non-invasive way to correct myopia.
The prescription, lens material, frame fit and intended daily use should be discussed with the practice performing the examination.
Contact lenses
Contact lenses can also correct myopia for suitable wearers.
Safe contact-lens use depends on:
- professional fitting
- correct cleaning and storage
- following the recommended replacement schedule
- not wearing lenses longer than advised
- seeking prompt assessment for pain, redness, light sensitivity or reduced vision
Refractive surgery
Some adults may be suitable for laser or other refractive procedures.
Suitability depends on factors such as:
- prescription stability
- corneal measurements
- age
- general health
- eye health
- realistic expectations about the procedure
Refractive surgery may reduce dependence on glasses or contact lenses, but it is not suitable for everyone. It also does not remove every eye-health risk associated with having a longer myopic eye.
Find Eye Care That Suits Your Needs
Search for an independent optometrist near you and find a local practice that suits your specific eye care needs.
Find an OptometristCorrection and myopia management are not the same
Standard glasses and contact lenses correct blurred vision.
Myopia management is a broader clinical approach that aims to reduce the rate of progression, particularly in children whose eyes are still growing.
An optometrist may discuss one or more of the following options for a child with progressing myopia:
- specialised spectacle lenses designed for myopia management
- specialised soft contact lenses
- orthokeratology lenses
- low-dose atropine eye drops prescribed and monitored as a medicine
- advice about outdoor time and near-work habits
- wearing the prescribed correction as directed
- regular reviews to assess vision, progression, eye health and treatment safety
No option is suitable for every child.
The decision may depend on:
- the child’s age
- the age when myopia began
- the rate of prescription change
- eye measurements
- the child’s daily activities
- the ability to manage contact-lens hygiene
- possible side effects
- family preferences
- costs and follow-up requirements
- the experience and services available at the practice
The goal is to slow progression. Myopia management cannot guarantee that progression will stop completely, and it does not reverse myopia that is already present.
Parents and carers can read the separate AMV guide to myopia management for children for more detail about treatment choices, monitoring and questions to ask.
Can myopia be prevented?
There is no reliable way to guarantee that a child will not develop myopia.
More time outdoors during childhood may reduce the risk of developing short-sightedness. Families can discuss suitable outdoor activity and sun protection with their healthcare professionals.
Near-work habits may also be considered, but no single screen rule or lifestyle change can replace an eye examination.
Children should still have vision concerns assessed even when they spend time outdoors and take regular breaks from close work.
Is Your Eye
Health on Track?
Complete our free 18-point checklist to check your eye health, spot any gaps, and take charge of your vision.
Start Free Checklist Test →Can myopia be reversed?
Once myopia is present, glasses and contact lenses can correct the focusing error and improve distance vision.
Evidence-based myopia management may slow further progression in children, but it does not reverse the existing myopia.
Claims that eye exercises, supplements, or unverified devices can cure myopia should be treated cautiously.
An optometrist can explain which options are supported by evidence and whether they may be appropriate for an individual child.
What is high myopia?
High myopia means a stronger degree of short-sightedness.
The clinical definition may consider prescription strength, the length of the eye or both.
A longer myopic eye can place more strain on tissues at the back of the eye. High myopia is therefore associated with a higher risk of retinal detachment and other myopia-related eye conditions.
This does not mean that every person with high myopia will develop a complication.
It does mean that regular eye-health examinations and clear instructions about sudden retinal symptoms are important.
People with high myopia should follow the monitoring schedule recommended by their optometrist or ophthalmologist.
When should you book an eye test?
Arrange a routine eye test when:
- distance vision is persistently blurred
- distance vision appears to be changing
- a child is squinting or moving closer to see
- a child is struggling with classroom or other distance tasks
- a current prescription no longer provides clear or comfortable vision
- a child’s prescription is changing and the family wants to discuss myopia management
- you have high myopia and are due for the monitoring recommended by your eye-care professional
Do not wait for a routine appointment if you experience sudden flashes, a sudden increase in floaters, a curtain or shadow across your vision, distorted vision or sudden vision loss.
Go to an emergency department immediately or call 000.
Questions to ask an optometrist
You may wish to ask:
- Is the blurred vision caused by myopia, or could another condition be contributing?
- Is the recommendation intended to correct the blur, slow progression, or both?
- What are the expected benefits and limitations of each option?
- What risks or side effects should we understand?
- How will changes in the prescription or the length of the eye be monitored?
- What symptoms should prompt an earlier review?
- What symptoms require urgent care?
- Does the practice provide the recommended service?
- Would referral or co-management with another practitioner be appropriate?
- What fees, follow-up appointments and replacement schedules should be expected?
Finding an independent optometrist
Persistent distance blur or concerns about a child’s vision can be discussed with an optometrist.
Services differ between practices, particularly for:
- childhood myopia management
- specialised contact lenses
- ocular biometry
- orthokeratology
- prescription medicines
- ongoing monitoring
Confirm the available services, fees and follow-up process directly with the individual practice.
Use the Australian Made Vision directory to view participating independent optometry practices.
Australian Made Vision provides general eye-health information and a directory. The individual practice provides examinations, prescriptions, clinical advice and care.
Find Eye Care That Suits Your Needs
Search for an independent optometrist near you and find a local practice that suits your specific eye care needs.
Find an OptometristFrequently asked questions about Myopia
Can myopia be cured or reversed?
Myopia can be corrected with glasses or contact lenses, and some adults may be suitable for refractive surgery. Current childhood myopia-management options aim to slow progression rather than reverse the condition or guarantee that it will stop.
Does wearing glasses make myopia worse?
Myopia can be corrected with glasses or contact lenses, and some adults may be suitable for refractive surgery. Current childhood myopia-management options aim to slow progression rather than reverse the condition or guarantee that it will stop.
Can screen time cause myopia in children?
Myopia does not have one simple cause.
Long periods of close work, including device use, and less time outdoors are associated with myopia risk. Family history, age of onset and eye growth also matter.
At what age does myopia stop changing?
There is no single age at which myopia stops progressing for everyone.
It commonly changes during childhood and adolescence, but it may continue to progress or first develop during early adulthood.
Monitoring should be based on the individual rather than a fixed age.
Is myopia the same as astigmatism?
No.
Myopia and astigmatism are different refractive errors. A person can have myopia, astigmatism or both.
An eye test measures the type and amount of correction required.
Can adults develop myopia?
Yes.
Although myopia commonly starts during childhood, it can also develop or continue progressing in early adulthood.
New or changing distance blur should be professionally assessed rather than self-diagnosed.
Can myopia cause blindness?
Most people with myopia can achieve clear vision with the correct glasses or contact lenses.
However, high myopia is associated with a greater risk of certain eye conditions, including retinal problems. Regular eye-health examinations can help monitor these risks.
Sudden flashes, new floaters, a curtain-like shadow or sudden vision loss require emergency assessment.
Australian Made Vision is an independent directory that helps patients find optometrists across Australia who may offer Australian-made spectacle lenses. We do not provide clinical services and recommend contacting practices directly to confirm the products and services they offer.
